The target volume is the primary tumor (tumor bed) and the affected nodes (respective lymphatic area in postoperative radiotherapy). Some authors recommend “prophylactic” irradiation of high-risk lymphatic nodes even in the absence of signs of tumorous affection in this area.
The regimes adequate for proton therapy, mainly in locally advanced NSCLC, allow increasing the individual doses per fraction and decreasing the total irradiation period (the same or higher biologically equivalent dose). The same fractionation regimen may be selected for central and peripheral tumours in early carcinomas due to the dosimetric advantages.
As respiratory movements may impair the correct and precise execution of proton irradiation, in the treatment of lung cancer we use the method of controlled breathing. This is achieved by the Dyn’R. The Dyn’R is a special spirometer which not only serves to monitor the breath, as is the case with a conventional spirometer, but also allows triggering of the radiation (radiation beam) only when inhaled to a certain breath level. The controlled breathing method has been chosen because it is important that the irradiated area of the body and the target volume of the tumor are irradiated the same way during each fraction. Since this irradiated volume varies depending on breathing, we need to ensure that the patient’s body is always in the same position. This is best done by holding their breath at a certain level.
This method makes it possible to minimize respiratory movements, and thus to irradiate the tumor with a high dose with maximum accuracy. At the same time, minimal irradiation reached the healthy part of the lung, other lung, heart, cardiovascular system and organs in the mediastinum. Proton therapy significantly increases the ratio between the chances of tumor control, i.e. increasing the effect of treatment and reducing possible serious side effects.
It is possible to conclude that proton radiotherapy ensures excellent dose distribution in patients with early-stage NSCLC, with high local control and survival rate. Patients with early-stage disease, centrally located tumors or those near the brachial plexus enjoy the greatest benefit from proton RT.
Table 1: Comparison of fractionation regimens in the treatment of localised/advanced NSCLC
Regimen
Dose (Gy)
Number of fractions/Dose per fraction (Gy)
Total duration (weeks)
Photons
74.0
37 x 2.0 Gy
7,4
Protons (locally advanced disease)
67.5
54.0
25 x 2,7 Gy
18 x 3 Gy
5
3,5
Protons (localized tumors)
60.0
70.0
10 x 6 Gy
10 x 7 Gy
2
2
Advantages of Proton Therapy
In early carcinoma treated with SBRT, proton therapy enables us to irradiate the target volume with less fields (in comparison with photon IMRT) and decrease the integral dose. Decreasing the integral dose is associated with lower risk of stochastic effects, i.e. lower risk of development of radiation pneumonitis, oesophagitis and secondary tumours. Furthermore, the dose for critical tissues decreases, mainly pulmonary tissue.
In locally advanced lung carcinoma, proton therapy is better than the photon therapy. It enables us to accelerate (shorten the total irradiation time), use lower number of treatment fractions (hypofractionation), decrease the total dose with maintaining or decreasing the toxicity (lower load of critical organs in the same dose in comparison with the phototherapy), thus providing higher quality of life for the patients. A further advantage is the lower integral dose when compared with photon irradiation, similarly to the early carcinoma.
Results with Proton Therapy
It has been demonstrated in patients with non-small cell lung cancer (NSCLC) that dose escalation improves local control and survival. Due to the physical properties (Bragg peak), minimization of the output dose occurs, leading to the sparing of critically important tissues such as heart, esophagus, airways, major vessels, and the spinal cord in comparison with photon radiation therapy. The reduction of toxicity in proton radiotherapy (PRT) leads to the reduced cost of the treatment of side effects, thereby reducing the cost of patient hospitalization. Dose optimization also makes it possible to spare healthy tissue in patients with complicated anatomical situations.
It is evident from recent works that proton radiotherapy is effective and safe in patients with centrally located stage I NSCLC. Furthermore, tumors located at the apex of the lung, close to the brachial plexus can be better irradiated by proton radiotherapy while sparing the surrounding healthy tissues. In patients with bilateral early stage NSCLC, better dose distribution is ensured when using proton radiotherapy compared to other therapeutic modalities. Several clinical studies have confirmed that proton radiotherapy ensures the delivery of the appropriate dose even in locally advanced disease. Prospective randomized studies show that improved local control during concomitant chemoradiotherapy improves the overall survival rate.
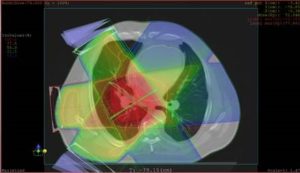
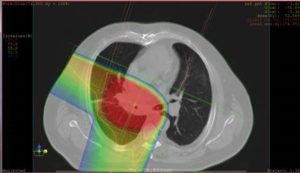
The following figure 1 and table 2 provide an example of irradiation schedule and dose distribution for individual organs. The slices in the planning CT scan show the dose distribution in the normal and tumorous tissue. In the proton therapy, only 1/6 of the dose in the tumour is administered to the right lung and the left lung is completely protected before the unwanted radiation.
photon IMRT radiotherapy
proton IMPT radiotherapy
Table 2: Doses tp lungs and spinal cord compared to the tumor dose
3-D RT (photons)
IMPT (protons)
Target volume (pulmonary tumor)
74 Gy (100%)
74 Gy (100%)
Lungs (Dmean)
19,7 Gy (26%)
8,8 Gy (11,8%)
Spinal cord (Dmax)
53 Gy (71%)
8,1 Gy (10,9%)
Book "Protonová radioterapie", author Pavel Vítek et al., published by Maxdorf